An Overview of Artificial Disc Replacement (ADR) for Cervical Spine
The artificial disc replacement (ADR) for cervical spine procedure could theoretically be used in any case where an anterior cervical decompression and fusion (ACDF) is used. There are mechanical advantages, disadvantages and limitations associated with this procedure.
The reason the artificial disc was invented initially was because degenerative disc disease can occasionally progress above and below the level of a cervical fusion. If some motion could be preserved, the levels adjacent might be spared further degeneration. Movement sparing devices can take some of the stress off of the levels above and below by preventing some increased forces that could cause degeneration.
Disc arthroplasty is designed to replace the motion of the damaged segment. It does so by restoring the height of the disc space and implanting bearing surfaces in place of the disc itself. Most disc replacements use titanium or chrome-cobalt alloys. The metal is designed to press fit into the disc space and the bone will either grow into the metal or attach to it by scar formation. The problem with this metal is it is not very MRI compatible. This does not mean that an MRI cannot be performed but the metal obscures the signal of the MRI around the area of the artificial disc replacement. Titanium is more ‘friendly” to MRI than chrome-cobalt is.
The replacement disc shares some of the characteristics of the biological disc but not all of them. The articulation or joint itself is a type of elongated ball and cup design. This design allows bending forward and backwards, side to side bending and some rotation. These designs will not allow shock absorption- an important component of a normal biological disc.
It turns out that genetics plays a big role in the determination of the health of a disc. There have been reports of degenerative changes above and below implanted artificial discs so the additional motion may not solve the dilemma of continuing degenerative changes.
Limitations of Artificial Disc Replacement
The artificial disc replacement (ADR) for cervical spine will not work in certain situations. The artificial disc replacement depends upon the vertebral segment other than the native disc to be intact to function properly. That is, the facets and the ligamentous connections have to be “normal”.
If the facets (the joints in the rear of the spine) exhibit degenerative changes such as wear of the cartilage surface, this could create pain with motion which is what the surgery is trying to avoid. If the facets have worn down enough to create a condition called a degenerative spondylolysthesis (where the vertebra above has shifted forward on the vertebra below) this instability would preclude using an artificial disc arthroplasty. If the disc space is diminished greater than 50%, the disc replacement has less chance of working as designed.
The long-term viability of the disc is not yet determined as these devices have not been around for more than 10 years. For artificial joints like a hip or knee, we know these joints will last 10 -15 years before they need to be replaced. Because of that wear pattern, artificial hip and knee joints tend to be implanted in individuals older than 60 years of age.
Disc replacements are being surgically implanted in younger adults and we do not know the life expectancy of the ADR at this point. Replacement procedures will have to be planned. The artificial disc in the cervical spine is generally easy to revise to a fusion if necessary.
Finally, some individuals, especially women, will develop osteoporosis as they age. The interface between the metal of the disc replacement and the bone of the vertebra may fail with advancing osteoporosis and the metal disc may subside into the bone.
Types of Artificial Disc Replacements
There are 2 main types of cervical disc implants- Medtronics Prestige LP, and Synthes Prodisc C.
The Prestige LP total disk replacement is made of titanium-ceramic composite which makes it somewhat better for MRI imaging. It has a ball-and-socket design. The entire disc is made of metal with the bearing surfaces entirely metal on metal. It attaches through a “fin and channel” into the endplate of the vertebra for initial stability and ingrowth surfaces for long-term stability. This is the only disc that is approved for a two adjacent-level procedure.
The ProDisc-C consists of two chrome cobalt alloy endplates (similar to stainless steel) with a plastic bearing surface fixed to the lower plate. The edges of the implant are attached to the vertebra by a central keel with an in-growth surface. The keel stabilizes the implant until bone growth occurs into the endplate.

(Click to Enlarge Image) Prestige LP artificial disc replacement-note the two keels on each half of the ADR and the “rough” flat surface on the top (and bottom) of this disc. This allows bony ingrowth from the vertebral body into the disc.

(Click to Enlarge Image) These are two Prestige LP artificial discs implanted in the front of the neck. You can see the “keels” imbedded in the bone and the small “rings” on either side of the disc that stabilizes these implants
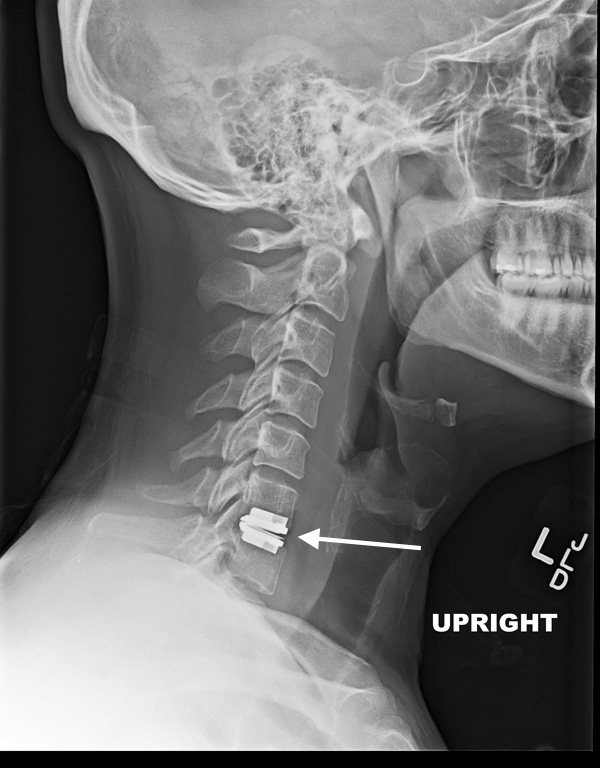
(Click to Enlarge Image) This is a lateral X-ray of a Synthes artificial disc replacement.
(Click to Enlarge Image) This is a Synthes artificial disc replacement at C6-7. The arrow points to the disc.

(Click to Enlarge Image) AP X-ray of a cervical artificial disc.
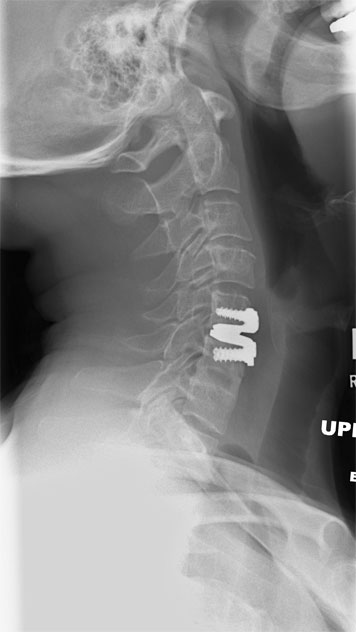
(Click to Enlarge Image) Lateral X-ray of cervical artificial disc in extension (bending backwards).

(Click to Enlarge Image) Lateral X-ray of cervical artificial disc in flexion (bending forwards). Note the motion in the disc from flexion to extension.
Are you a candidate for artificial disc replacement (ADR)?
Would you like to consult with Dr. Corenman about your condition?
You can set up a long distance consultation to discuss your
current X-rays and/or MRIs for a clinical case review.
(Please keep reading below for more information on this treatment.)
The differences in the two discs are not significant for a one level surgery (except for MRI compatibility) but do become significant with more than one level disease. The only approval currently for 2 ADRs in a row in a cervical spine is the Prestige LP disc. If a fusion (an ACDF) is needed in conjunction with an ADR for more than one level of disease, the Prestige LP and ProDisc-C will allow fixation of the ACDF level with a plate. This would allow a better chance of healing for the fusion level. Using a Prestige disc will not allow a plate to be used in an adjacent vertebra.
If two ProDisc-C ADRs are used next to each other (such as at C5-6 and C6-7), the keels that attach the disc to the vertebra can act as a wedge and possibly split the vertebral body in-between with significant impact.
Dr. Donald Corenman, spine surgeon and neck specialist, welcomes new patients at his practice. To learn more about the artificial disc replacement (ADR) for cervical spine procedure as a treatment option for spine related conditions, please contact Dr. Corenman at his Vail, Aspen, Denver and Grand Junction, Colorado area office.
Related Content
- How to Describe Your History and Symptoms of Neck, Shoulder and Arm Pain
- Best Questions to Ask When Interviewing a Spine Surgeon or Neurosurgeon
- When to Have Neck Surgery
- Anterior Cervical Decompression & Fusion (ACDF)
- Cervical Laminectomy, Laminoplasty and Posterior Cervical Fusion
- Posterior Cervical Foramenotomy
- Myths of Laser Spine Surgery